By Peg Coleman, MS, MS
In my recent Wise Traditions article (Spring 2023),1 I wrote about Microbial Risk Assessment (MRA), a qualitative or quantitative structured approach developed by international consensus.2 Overall, the approach would begin with the best available data at the time, consider alternative assumptions where uncertainty existed about model parameters, and conclude with reporting risk estimates with uncertainty, data gaps and limitations.
Uncertainty and data gaps are crucial to address because data are rarely sufficient to estimate risk without invoking assumptions where data are sparse, inconsistent, of a poor quality, ambiguous or conflicting. An MRA can be considered a snapshot in time for a given set of data and assumptions. Targeted research may be conducted to fill significant data gaps. As scientific knowledge advances, earlier data and assumptions may prove invalid, and the MRA would require updating, consistent with international principles and guidelines.2
One common and crucial misunderstanding that I address in this article the fact that epidemiology is not risk assessment as defined by international consensus.2 Epidemiologic data are generally used for two major purposes in MRA, starting with the first MRA element: identifying which pathogens present in foods have the potential to cause adverse human health effects (hazard identification). Consistent with the work of Abe and colleagues,3 I report numbers of illnesses rather than numbers of outbreaks due to higher relevance for representing the burden of illness for risk management decisions.
CURRENT DATA ON HAZARD IDENTIFICATION
For the purposes of this article, I use a Centers for Disease Control and Prevention (CDC) data set for 2005 through 2020,4 comparing the CDC data with global data considered by the European Food Safety Authority (EFSA) and European Union (EU) opinions about hazards associated with raw milk.5 According to the CDC data (Figure 1), the major pathogen causing illness associated with raw milk for the sixteen-year period was Campylobacter (1,570 illnesses, including one death in a case with chronic underlying disease). In addition, Campylobacter was associated with 1,647 pasteurized milk illnesses, for a total of 3,217 illnesses. Note that although parasites caused some milk-borne illnesses in the U.S. in this time period (sixty-two cases of cryptosporidiosis; thirty-eight cases of giardiasis), this article emphasizes bacterial illnesses.
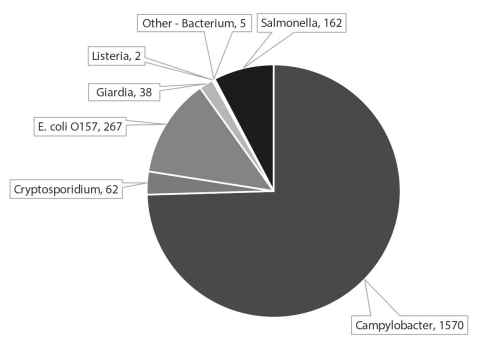
FIGURE 1. Pathogens associated with raw milk (CDC, 2005-2020).
As a microbiologist, it is puzzling to me that the major milk-borne hazard, campylobacteriosis, was associated with 3,217 illnesses, yet the pathogen cannot actually grow at refrigeration temperatures in raw or pasteurized milk. Neither can Campylobacter grow under normal aerobic conditions for culturing. Recent studies document promising results for chemical, phytochemical and microbial interventions that can disrupt persistent Campylobacter biofilms that might be the root cause for milk-borne illnesses.6-9 Other major foods that also contributed to the burden of campylobacteriosis in this time period included:
- Poultry (603 illnesses
- Mollusks (408 illnesses)
Moderate numbers of illnesses associated with raw milk outbreaks were reported for pathogenic E. coli (267 illnesses, zero deaths) over the sixteen-year period. Other foods contributed to the majority of the burden of pathogenic E. coli cases, including:
- Leafy-vine-stalk vegetables (2,221 illnesses)
- Beef (1,485 illnesses)
Moderate numbers of illnesses associated with raw milk outbreaks were reported for salmonellosis (162 illnesses, zero deaths) over the sixteen-year period. Other foods contributed to the majority of the burden of salmonellosis cases, including:
- Poultry (6,244 illnesses)
- Leafy-vine-stalk vegetables (6,000 illnesses)
- Pork (2,759 illnesses)
- Beef (1,715 illnesses)
- Melons (1,544 illnesses)
- Root/underground vegetables (1,540 illnesses)
- Processed nuts (1,490 illnesses)
- Sprouts (983 illnesses)
The smallest hazard associated with raw milk in this period was two Listeria monocytogenes illnesses; one of the two individuals was immunocompromised and died10. Multiple lines of evidence support the success of existing risk management controls (such as proper refrigeration,5 hazard analysis and critical control points or risk analysis and management plans11 and proper hygiene in milk parlors) in limiting listeriosis cases associated with raw milk.
These recent CDC data for raw milk hazards are consistent with the 2015 findings of the EFSA,5 which reported that major bacterial hazards included Campylobacter, pathogenic E. coli and Salmonella, but not listeriosis.
Hazard identification for pasteurized milk differs in that a recent systematic review for North America documented four deaths and a higher risk of hospitalization and death from listeriosis associated with pasteurized, not raw, milk.12
Other foods that contributed to the majority of the burden of listerioisis cases in the U.S. were:
- Melons (153 illnesses)
- Pasteurized solid/semi-solid dairy (73 illnesses)
- Pome, stone, and sub-tropical fruits (54 illnesses)
- Deli meats (49 illnesses)
- Leafy-vine-stalk vegetables (48 illnesses)
- Fungi (41 illnesses)
- Raw solid/semi-solid dairy (37 illnesses)
Considering foodborne deaths, we have just seen that one death each from campylobacteriosis and listeriosis over the sixteen-year period were attributed to raw milk. Note that in this period, 141 other deaths were attributed to Listeria monocytogenes. Foods other than raw milk were associated with 75 deaths from salmonellosis and 40 deaths from pathogenic E. coli.
Overall, considering the CDC data for 2005-2020 in the Hazard Identification phase of MRA, neither raw nor pasteurized milks are risk-free, and both are associated with bacterial hazards that, under certain conditions, may contribute to risk of foodborne illness. Both raw and pasteurized milk were rarely associated with fatalities, though five were reported in the sixteen-year period, two associated with raw milk and three with pasteurized milk. Note that some illnesses and deaths were also associated with other raw and pasteurized dairy products in this period as documented in the previous bullets, though I do not report on these data further in this article.
DATA FOR EXPOSURE ASSESSMENT
Microbiology, not epidemiology, provides the major source of evidence for the MRA element exposure assessment, notably data on the presence or absence of pathogens in raw milk and pathogen growth or decline during storage. Another common and crucial misunderstanding addressed herein is the fact that data on the presence or absence of pathogens, or levels of indicator microbes (such as total plate counts, coliforms and generic E. coli), are insufficient evidence to estimate microbial risk. The more important determining factors in predicting both the chance or likelihood of illness and the severity of illness are the levels or densities of pathogens and natural microbiota, and whether or not pathogen growth occurs under typical storage conditions of the food.
Some significant shortfalls in MRA quality were identified in the exposure assessment of the MRA on severe listeriosis associated with twenty-three ready-to-eat foods including raw and pasteurized milks.13 Colleagues in the Society for Risk Analysis (SRA), Applied Risk Management specialty group developed the Risk Analysis Quality Test (RAQT)14 that I applied to both MRAs considering milk prepared by FDA/FSIS (2003)13 and FSANZ.15
The exposure assessment for milk-borne listeriosis by the two U.S. agencies—the Food and Drug Administration (FDA) and the Food Safety and Inspection Service (FSIS)—was based on sparse data and invalid assumptions. The Agencies assumed that quality and safety of pre-pasteurized milk (that is, milk from multiple farms in bulk tanks and regional silos stored for unspecified periods prior to pasteurization) was equivalent to that of fresh raw milk from farms producing raw milk for direct human consumption.
FDA presented results of their recent systematic review on prevalence of pathogens in raw milks at the International Association for Food Protection conference in Toronto this year.16 Not surprisingly, the prevalences of pathogens in pre-pasteurized milk greatly exceeded prevalences from government monitoring programs for dairies producing raw milk for direct human consumption.17
The agencies also assumed that pathogen growth was equivalent in raw and pasteurized milk, though a cited study reported contrary results18 (no growth or lower growth in raw milk). Further, a manuscript on analysis of results from a 2022 pilot study on growth of the four major pathogens in raw milk produced for direct human consumption was accepted by PLOS ONE in July of 2023.19 This study documents suppression of pathogen growth at 4.4 °C over the fourteen-day storage period for all three major pathogens identified as hazards raw milk in the U.S. in the previous hazard analysis section.
RISK ANALYSIS QUALITY TEST OF SRA
A half-day workshop and a round table panel symposium were conducted at the SRA conference in Tampa on beta testing of the Risk Analysis Quality Test (RAQT) for milks. WAPF leader Pete Kennedy participated in the 2022 SRA workshop in Tampa where the beta testing results for the MRAs were discussed.
Prior to the round table, a panelist, former FDA economist Richard Williams recalled a closed-door internal FDA meeting where the draft MRA results were shared with management. Even though pasteurized milk was classified as a high-risk food, as noted in the Summary Table (page 95), a decision was made that consumers were not going to be warned about risks of consuming pasteurized milk. The language of the final 2003 MRA document reflected this pro-pasteurization bias clearly, describing the decision that set separate courses for risk management of raw milk (“priority candidate for continued avoidance”) and pasteurized milk (“priority candidate for more study to confirm model predictions or identify factors not captured by current models that would reduce risk”).
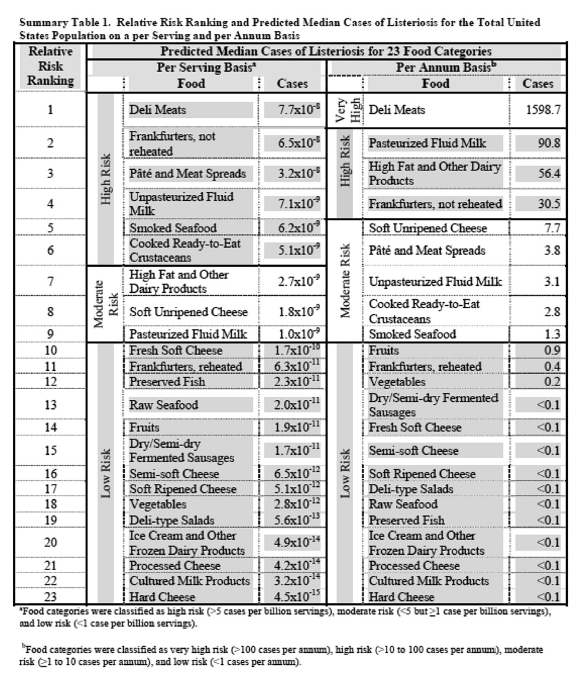
Summary Table 1: Relative Risk Ranking and Predicted Median Cases of Listeriosis for the Total United States Population on a per Serving and per Annum Basis.
The basis for assigning “avoidance” and “more study” to two foods both ranked as high risk was not specified in the assessment. In my view, both commodities merit more study and updating of the risk assessment based on data and assumptions more than twenty years old. Re-evaluation in light of more than a decade of scientific advances characterizing the microbiota of milks would be in keeping with the general principles for MRA.2
Based on the set of data and assumptions considered by FDA and FSIS at the time, the agencies reported risk as both per serving estimates and annual estimates of severe illness. Both are estimates that together characterize risk that may inform decision-making. In the Summary Table’s left column on a per-serving basis, the agencies ranked raw milk fourth highest of the twenty-three food groups considered, and pasteurized milk ninth highest. In the right column on a per annum basis, the agencies ranked pasteurized milk second highest and raw milk ranked seventh highest.
It is notable that FDA manager John Sheehan excluded citation of the 2003 FDA/FSIS ranking of both raw and pasteurized milk as high risk for severe listeriosis from his affidavits for the Toronto case in 2018 and 2019. Nor did he acknowledge FDA/FSIS assignments of different risk management actions for raw and pasteurized milks that strongly suggest a pro-pasteurization bias. The discussions about RAQT results at the SRA meeting considered the CDC dataset for 2005-2020 and data from the recent decade of advances in knowledge of the microbiota of milks.20
REASSESSING RISK WITH INDEPENDENT EPIDEMIOLOGIC DATA AND SCIENTIFIC ADVANCES
The final two general principles of MRA2 are of great relevance to global societies: risk estimates should be reassessed over time by comparison with independent epidemiologic data on human illness; and MRAs may need reevaluation as new relevant scientific data become available.
Many microbial risk assessment teams use epidemiologic evidence as a reality check at the end of the MRA process to compare the numbers of annual illnesses estimated from their risk models with the numbers actually observed over time from human disease surveillance programs. If inconsistencies are significant, the MRA data and models might be reexamined, the MRA results may be flagged as uncertain (low confidence), or additional data might be collected to replace assumptions for future reevaluation of the MRA.
The FDA/FSIS MRA Summary Table 1, opposite, lists estimates of high risk for per serving associated with raw milk (seven serious listeriosis cases per one hundred million servings) and moderate risks (three serious listeriosis cases per year). Now, compare the FDA/FSIS MRA annual estimate with subsequent epidemiologic data on listeriosis from the CDC dataset for 2005-2020:
- MRA estimate: three serious listeriosis illnesses per year (2003)
- CDC reported cases: two listeriosis illnesses over sixteen years (2021)
If the MRA estimate represented current data, one might expect approximately forty-eight cases in the subsequent sixteen-year period, not two. Also, in fifteen of sixteen years, no listeriosis cases were observed associated with raw milk. Clearly, subsequent CDC data are inconsistent with the FDA/FSIS ranking of moderate risk per annum for raw milk or of the FDA position that raw milk is inherently dangerous.
The high risk ranking for listeriosis in raw milk per serving from the 2003 FDA/FSIS assessment is also inconsistent with subsequent reassessments of independent academic teams that estimated lower risk for raw milk21 and higher risks associated with increasing temperatures for pasteurizing milk.22
Granted, uncertainty may be high in both MRA simulations and epidemiologic data.
Based on international consensus on general principles,2 the epidemiologic evidence and the protective effects against infectious pathogens18 and non-communicable disease17 support the need for updating the milk FDA/FSIS MRA (2003),10 as well as the MRA subsequently prepared by FSANZ (2009).15
Moreover, trends since 2005 in raw milk outbreaks and illnesses across all bacterial pathogens are flat or declining, not increasing, for both the U.S. overall and for each U.S. state (manuscript under review). In fact, Figures 2 and 3 (below) document the fact that retail raw milk production in California and numbers of raw milk licenses approved by New York state are increasing in this time period, while raw milk outbreak numbers and rates are flat or declining. This is exactly contrary to what would be expected if access to raw milk was linked to increasing numbers of outbreaks and illnesses.
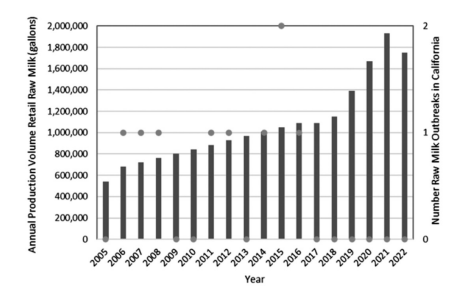
FIGURE 2: California retail raw milk production from one licensed dairy and state outbreaks by year.
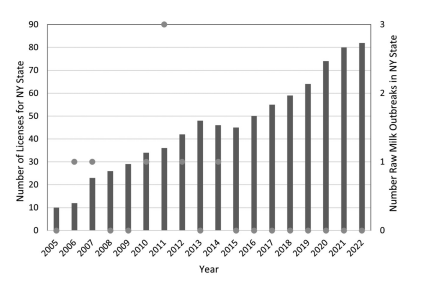
FIGURE 3: New York state licenses for raw milk dairies and outbreaks by year.
Milks, both raw and pasteurized, are not risk-free. For the most recent eighteen years of data from the U.S. CDC (2005–2020, NORS Access dataset; 2021-2022, NORS online Dashboard), the state of California reported a total of six outbreaks, eighty-three illnesses, eleven hospitalizations, and no deaths associated with raw milk. Of those eighty-three illnesses, sixty-eight were campylobacteriosis and fifteen were due to pathogenic E. coli O157:H7. One California producer (Raw Farm, formerly Organic Pastures) sold nearly nine million gallons of retail raw milk from 2017 to 2022, without a single outbreak reported in the state linked to raw milk consumption. This volume of raw milk in the California retail market represents a risk of infectious illness of less than one in twenty million 250-mL servings.
For New York, the most recent eighteen years of data (2005–2022), a total of eight outbreaks, fifty-eight illnesses, four hospitalizations, and no deaths were reported. All those fifty-eight illnesses were campylobacteriosis. No raw milk consumers became ill from other pathogens—which caused more hospitalizations (and deaths) from consuming leafy greens!
The available evidence is consistent with adequacy of current hygienic procedures and cold-chain for raw milk producers, which minimizes risk of illness and enhances safety for listeriosis, perhaps illnesses from pathogenic E. coli and Salmonella, but not for Campylobacter. The burden of campylobacteriosis for both raw and pasteurized milks warrants further study and evaluation, particularly regarding technologies to disrupt biofilm formation.6-9 We note the societal need for cultivating a culture of quality analysis in governmental MRA projects and support updating the 2003 and 2009 MRAs for raw milk.
Margaret E. (Peg) Coleman, MS, MS, is a medical microbiologist, a microbial risk analyst, and a fellow of the Society for Risk Analysis (SRA). Her long career in microbial risk analysis began with the U.S. federal government (USDA/FSIS and ARS) and continues as a consultant. Her primary interests are benefit-risk analysis, resilience of human superorganisms and humans’ microbial partners in health.
ACKNOWLEDGEMENTS
WAPF provided support for preparation of this article, structuring of the CDC Access database and travel to the International Food Protection (IAFP) conference in Toronto. Also appreciated is ongoing support from: Michele Stephenson for querying the CDC Access database and generating figures; and Sally Fallon Morell of WAPF, Mark McAfee of RAWMI, and Abby Rockefeller of Churchtown Dairy. Mark and Abby recently supported a contract with an independent laboratory for conducting the pilot study on pathogen growth and decline, as well as provided support for further analysis of the pilot study data and preparation of the manuscript on that analysis.
REFERENCES
1. Coleman P. Raw milk risks from a microbiologist’s perspective. Wise Traditions. Spring 2022;23(1):101-105.
2. Codex Alimentarius Commission (CAC). Principles and guidelines for the conduct of microbiological risk assessment. CAC/GL-30 (1999). https://www.fao.org/3/y1579e/y1579e05.htm
3. Abe H, Garre A, Koseki S, et al. Analysis of a quantitative risk assessment of listeriosis from pasteurized milk: the combinations of which factors cause listeriosis in this low-risk food? Food Control. 2023;152:109831.
4. Centers for Disease Control and Prevention. Access® database for outbreaks reported from 2005 to 2020 from all transmission sources (food, water, animal contact, environmental and person-toperson) provided by Hannah Lawinger, CDC NORS Data Request Manager to author on May 26, 2021. Note that data on numbers of illnesses for food groups reflected records from the Access® database with both IFSAC-3 and IFSAC-4 data.
5. EFSA Panel on Biological Hazards. Scientific Opinion on the public health risks related to the consumption of raw drinking milk. EFSA Journal. 2015;13(1):3940.
6. Wagle BR, Upadhyay A, Upadhyaya I, et al. Trans-cinnamaldehyde, eugenol and carvacrol reduce Campylobacter jejuni biofilms and modulate expression of select genes and proteins. Front Microbiol. 2019;10:1837.
7. Elgamoudi BA, Korolik V. Campylobacter biofilms: potential of natural compounds to disrupt Campylobacter jejuni transmission. Int J Mol Sci. 2021;22(22):12159.
8. Mgomi FC, Yuan L, Chen CW, et al. Bacteriophages: a weapon against mixed‐species biofilms in the food processing environment. J Appl Microbiol. 2022;133(4):2107-2121.
9. Lavilla M, Domingo-Calap P, Sevilla-Navarro S, et al. Natural killers: opportunities and challenges for the use of bacteriophages in microbial food safety from the One Health perspective. Foods. 2023;12(3):552.
10. Nichols M, Conrad A, Whitlock L, et al. Short communication: Multistate outbreak of Listeria monocytogenes infections retrospectively linked to unpasteurized milk using whole-genome sequencing. J Dairy Sci. 2020;103(1):176-178.
11. Raw Milk Institute. Risk Analysis and Management Plan. https://www.rawmilkinstitute.org/common-standards.
12. Sebastianski M, Bridger NA, Featherstone RM, et al. Disease outbreaks linked to pasteurized and unpasteurized dairy products in Canada and the United States: a systematic review. Can J Public Health. 2022;113(4):569-578.
13. Center for Food Safety and Applied Nutrition, Food Safety and Inspection Service. Interpretive Summary: Quantitative Assessment of the Relative Risk to Public Health from Foodborne Listeria monocytogenes Among Selected Categories of Ready-to-Eat Foods. U.S. Food and Drug Administration and U.S. Department of Agriculture, September 2003. https://www.fda.gov/food/
cfsan-risk-safety-assessments/quantitative-assessment-relative-risk-public-health-foodbornelisteria-monocytogenes-among-selected
14. https://www.sra.org/risk-analysis-specialty-groups/applied-risk-management/scientific-literature/
15. Food Standards Australia New Zealand. Microbiological Risk Assessment of Raw Cow Milk. Risk Assessment Microbiology Section, December 2009. https://www.foodstandards.gov.au/code/proposals/documents/p1007%20ppps%20for%20raw%20milk%201ar%20sd1%20cow%20milk%20risk%20assessment.pdf
16. Williams EN, Van Doren JM, Leonard CL, et al. Prevalence of Listeria monocytogenes, Salmonella spp., Shiga toxin-producing Escherichia coli, and Campylobacter spp. in raw milk in the United States between 2000 and 2019: a systematic review and meta-analysis. J Food Prot. 2023;86(2):100014.
17. Dietert RR, Coleman ME, North DW, et al. Nourishing the human holobiont to reduce the risk of non-communicable diseases: a cow’s milk evidence map example. Appl Microbiol. 2022;2(1):25-52.
18. Northolt MD, Beckers HJ, Vecht U, et al. Listeria monocytogenes: heat resistance and behaviour during storage of milk and whey and making of Dutch types of cheese. Neth Milk Dairy J. 1988;42:207-219.
19. Coleman ME, Oscar PT, Negley TL, et al. Suppression of pathogens in properly refrigerated raw milk. PLOS One. Forthcoming (accepted July 2023).
20. Oikonomou G, Addis MF, Chassard C, et al. Milk microbiota: what are we exactly talking about? Front Microbiol. 2020;11:60.
21. Latorre AA, Pradhan AK, Van Kessel JAS, et al. Quantitative risk assessment of listeriosis due to consumption of raw milk. J Food Prot. 2011;74(8):1268-1281.
22. Stasiewicz MJ, Martin N, Laue S, et al. Responding to bioterror concerns by increasing milk pasteurization temperature would increase estimated annual deaths from listeriosis. J Food Prot. 2014;77(5):696-712.